HD Auswertung England
Da oftmals gefragt wird, was die Zahlen bei der HD Auswertung in England zu bedeuten haben, habe ich einige Informationen zusammen gesucht, die dies sehr gut erklären.
Ich habe sie nicht ins Deutsche übersetzt, denke aber, dass das Wesentlich gut verständlich ist.
In England wird jede Seite einzeln beurteilt, pro Seite werden 9 Kriterien untersucht und mit Punkten von 0-6 (Ausnahme Hintere Acetabulum Begrenzung die nur 0-5) bewertet.
Je weniger Punkte, desto besser. Zusätzlich wird in England ein Mittelwert (BMS) der einzelnen untersuchten Rassen gebildet (beim Beardie beträgt er momentan 11).
Ich habe auch eine Tabelle beigefügt, in der die Bewertungen von Deutschland, der Schweiz, England, Schweden, Finnland, den Niederlanden und den USA aufgeführt sind und somit der Vergleich erleichtert wird. Ich möchte aber darauf hinweisen, dass es sich hierbei nur um eine Zusammenstellung handelt und nicht um einen von der FCI festgelegten Vergleich.
Hip Scoring
The British Veterinary Association (BVA) and The Kennel Club in the UK (TKC) have joined together to run a hip scoring scheme for breeders, in order to test for canine hip dysplasia, the most common inherited joint problem of large breed dogs. This current system came into effect in 1984.
Dogs are scored from the age of 12 months, and can only be scored once in their lifetime.
The BVA/TKC publish a list of Breed Mean Scores (BMS) for each breed, together with the number of dogs tested to date and the range of scores achieved. It is then recommended that breeders ensure their breeding stock have scores which are well below the BMS.
From an x-ray taken at the owner's vets, the BVA scores each of the hip joints:
1. the norberg angle (0-6);
2. subluxation (0-6);
3. cranial acetabular edge (0-6);
4. dorsal acetabular edge (0-6);
5. cranial effective acetabular rim (0-6);
6. acetabular fossa (0-6);
7. caudal acetabular edge (0-5);
8. femoral head and neck exostosis (0-6);
9. femoral head recontouring (0-6),
thus each hip can receive a maximum score of 53 and overall score of 106. The lower the score the better, so 0/0 would be perfect, while 53/53 would mean that the dog had no hips at all!
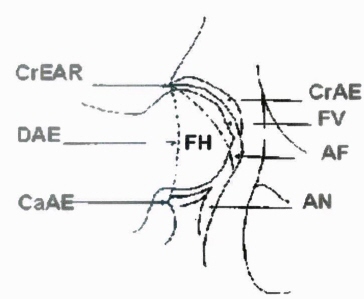 Diagram shows scores of 0.
Diagram shows scores of 0.
AF - Acetabular fossa
AN - Acetabular notch
FH - Femoral head
FV - Foveal defect
DAE - Dorsal Acetabular edge
CaAE - Caudal acetabular edge
CrAE - Cranial acetabular edge
CrEAR - Cranial effective acetabular rim
Norberg Angle
Measures two features - the degree of congruence between the FH and acetabulum and the length of the CrAE which gives a relative indication of acetabular depth.
Subluxation
Evaluation is based principally on the degree of congruence between the femoral had and acetabulum. The general 'fit' of these two components is assessed by the relationship between the FHC and the underlying image of the DAE; the configuration of the cranial joint space is also taken into account, particularly at the lower end of the scoring scale, when abnormalities are relatively minor. The cranial joint space is seen as a radiolucent shadow between the CrAE and adjacent cranial articular margin of the FH. For a zero score the FHC must be medial to the DAE and the cranial joint space uniformly narrow, with the curve of the CrAE eactly following that of the FH.
Cranial Acetabular Edge
Minor alterations in the shape, contour and possibly the length of the CrAE are generally believed to be indicators of poor articular congruence, while more severe changes are clearly consequences of chronic instability, abnormal marginal wear and remodelling of the joint. For a score of zero the CrAE should be convex, uniformly curved and match exactly the countour of the adjacent femoral head with no lateral or medial divergence of the cranial joint space.
Dorsal Acetabular Edge
On good quality radiographs, the DAE forms a well-defined density interface which traverses the fH almost vertically and extends a little beyong it cranially and caudally. The clarity whith which it can be seen is highly variable. A minor change in the contour of the DAE, which is normall slightly curved, merits a score of 1, but small localised irregularities, seen only on radiographs of exceptionally high quality, are considered to be within normal limits. Higher scores are related to definitive pathological changes associated with degenerative joint disease (osteoarthritis), the smallest being minor exostosis, which is usually seen cranially.
Cranial Effective Acetabular Rim
The earliest detectable abnormalities of the CrEAR are either minor exostosis, usually in the form of a small, well-modelled osteophyte, or slight 'rounding off' of the junction between the CrAE and DAE, which may be seen in the presence of a non-biblabiated CrAE.
Acetabular Fossa
Detectable bone deposition in the AF is almost always associated with marked subluxation and the amount tends to increase in proportion with the increase in the other radiographic hallmarks of secondary degennerative joit disease (osteoarthritis). Objective numerical scoring of this criterion is difficult, but as changes are likely to be recorded only in dogs with a total score considerably higher han average, the importance of a high level of accuracy is diminished.
Caudal Acetabular Edge
The CaAE is the segment of the acetabulum which is subject to the widest range of normal radiographic variation. Radiographic abnormalities are scored between 0 and 5 and changes are due mainly to exostosis with signs of wear being apparent only in advanced cases.
Femoral Head and Neck Exostosis
The normal FH should have a smooth rounnnnndish profile, but the shape may vary considerably.
Recontouring of the Femoral Head
This criterion is used to record the extent to which the FH shape is altered as a consequence of instability. Thus scores are likely to be awarded only in cases in which secondary changes are well established, when remodelling occurs as a result of the combined effects of periarticular new bone formation and loss of subchondral bone following total destruction of articular cartilage.
Scoring Criteria:
| Score | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
| Norbert Angle | +15° and over | +10° to +14° | =5° to +9° | 0° to +4° | -1° to -5° | -6° to -10° | -11° and over |
| Subluxation | Femoral head well centred in acetabulum | Femoral head centre lies medial to DAE. Lateral or medial joint space diverges slightly |
Femoral head centre superimposed on DAE. Medial joint space increase obvious | Femoral head centre just lateral ti DAE. 1/2 femoral head within acetabulum | Femoral head centre clearly lateral to DAE. | Femoral head centre well lateral to DAE. Femoral head just touches DAE | Complete pathological dislocation |
| Cran. Acetabulum Edge CrAE |
even curve, parallel to femoral head troughout | Lateral or medial 1/4 CrAE flat. Lateral or medial joint space diverges sligjtly |
CrEA flat throughout most of its length | CrAE shows slight bilabiation | 1/4 femoral head within acetabulum | CrAE shows gross bilabiation | Entire CrAE slopes cranially |
| Dorsal Acetabulum Edge DAE |
DAE has slight surve | Loss of S-curve only in the presence of other dysplastic change | Very small exostosis on cran. DAE | Obvious exostosis on DAE; especially cran. and/or minor "loss if edge" | CrAE shows moderate bilabiation | Marked exostosis all along DAE and/or gross "loss of edge" | Masive exostosis from cranial to caudal DAE |
| Cran. Effective Acetabulum Rim Cr.EAR |
Sharp, clear-cut junction of DAE & CrAE | Indistinct junction of DAE & CrAE | Very small exostosis or very small facet | Facet and/or small exostosis and/or slight bilabiation | Exostosis well lateral to DAE and/or moderate "loss of edge" | Gross exostosis and/or facet and/or gross bilabiation | Complete remodelling of CrEAR. Massive exostosis and/or gross facet |
| Acetabular Fossa AF |
A fine bone line curves medial and caudal from causal end of CrEA | Slight increase in bone density medial to AF. "Fine line" hazy or lost | Fine line lost ind AF and vetral AF hazy due to new bone. Notch at CaAE clear | Incomplete remodelling of acetabulum with medial face lateral to AF. Ventral AE lost. AF hazy. Notch irregular | Obvious facet and/or obvious exostosis and/or moderate bilabiation | Gross remodelling. Dense new bone troughout acetabulum. CaAE notch lost and AF obscurred | Complete remodelling and new articular surface, well lateral ti AF. Notch lost |
| Caudal Acetabular Edge CaAE |
Clean line | Small exostosis at lateral CaAE | Small exostosis at lateral an medial CaAE | Large exostosis an narrow notch at CaAE | Marked exostosis and "hooking" of lateral end of CaAE | Gross distorsion due to mass of new bone in acetabulum. Notch completely lost | Void |
| Femoral Head/Neck Exostosis | Smooth rounded profile | Slight exostosis in "ring form" and/or dense vertical bony line adjacent to trochanteric Fossa ("Morgan Line") | Slight exostosis visible on skyline and/or density on medial femoral head. | Distinct exostosis in "ring formation" | Obvious complete collar of exostosis | Massive exostosis giving mushroom appearance | Massive exostosis and infill of trochanteric fossa and below femoral head |
| Femoral Head Recontouring | Nil | Femoral head does not fit in circel due to exostosis or bone loss. | Some bone loss and/or femoral head/neck ring of exostosis | Obvious loss and distinct exostosis giving slight conical appearance | Gross remodelling. Obvious bone loss and exostosis gives mushroom appearance | Very gross remodelling with marked bone loss and much new one | Femoral head improperly shaped due to maldevelopment or femoral head centre |
Internationaler Vergleich der Einteilung bei HD
|
|
Deutschland | UK Sum / one joint |
Schweiz | Schweden | USA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
one joint 9-12 |
|
|
|
|
|
|
one joint 13-18 |
|
|
|
|
|
|
one joint >18 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|